
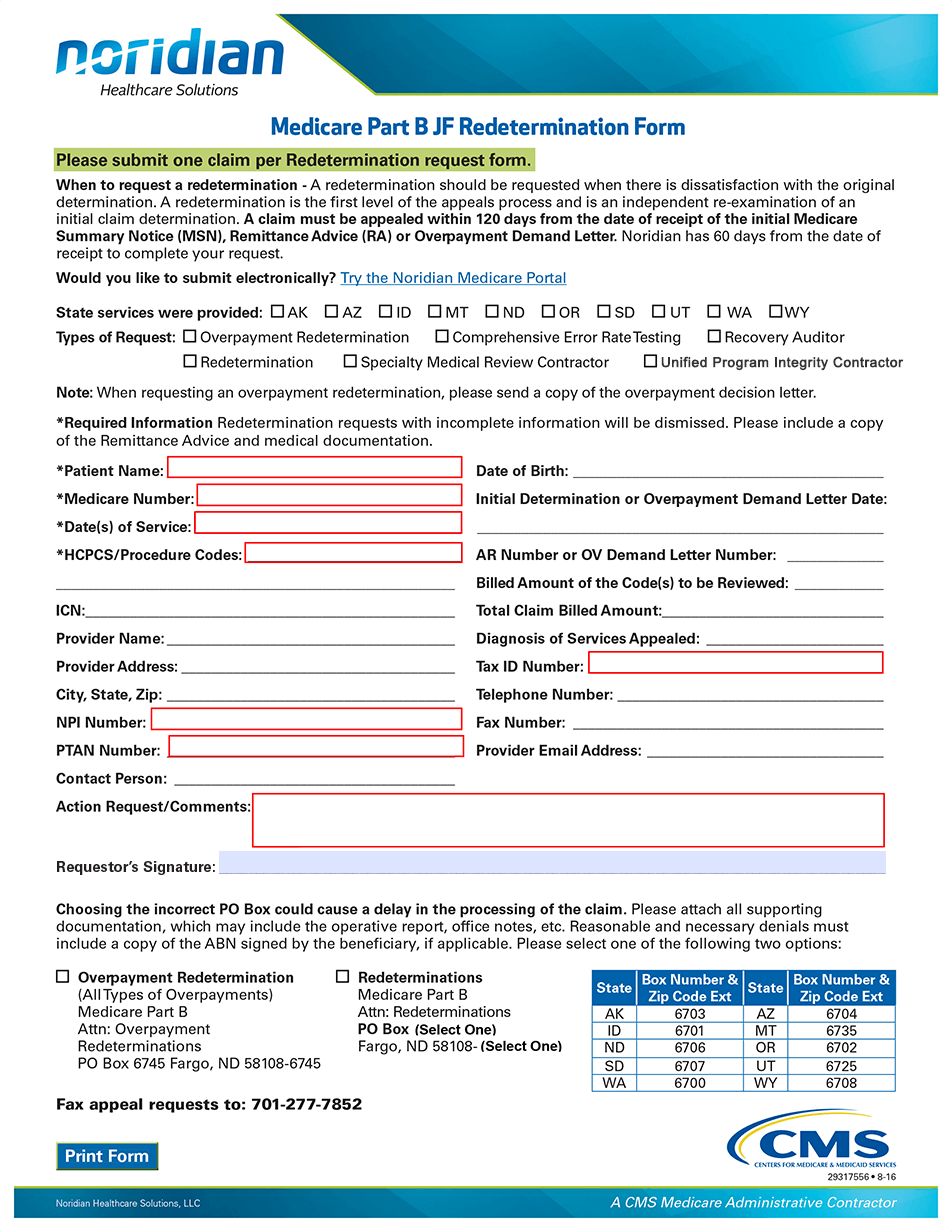
Medicare Part B Redetermination Form
Medicare Part B Redetermination Form - Please attach the evidence to this form or attach a statement explaining what you intend to submit and when you intend to submit it. You may also submit additional evidence at a later time, but all evidence must be received prior to the issuance of the redetermination. Please complete each field on the form to ensure accurate processing. Medicare redetermination request form department of health and human services centers for medicare & medicaid services 1. The appellant should include with their redetermination request any and all documentation that supports their argument against the previous decision. Do not complete this form for the following situations: Please attach the evidence to this form or attach a statement explaining what you intend to submit and when you intend to submit it.
Do not complete this form for the following situations: Transferring your appeal rights to your provider or supplier so they can file an appeal if medicare decides not to pay for an item or service. Please complete and mail this form with all pertinent documentation (medical records, certificate of medical necessity, operative notes, advance beneficiary notice of noncoverage, etc.). Please attach the evidence to this form or attach a statement explaining what you intend to submit and when you intend to submit it.
Medicare part b je redetermination form please submit one claim per redetermination request form. Do not complete this form for the following situations: Medicare part b redetermination and clerical error reopening request form. Please attach the evidence to this form or attach a statement explaining what you intend to submit and when you intend to submit it. There are 2 ways that a party can request a redetermination: You may also submit additional evidence at a later time, but all evidence must be received prior to the issuance of the redetermination.
Fillable Online Medicare Part B Jurisdiction 15 Redetermination Request

Transferring your appeal rights to your provider or supplier so they can file an appeal if medicare decides not to pay for an item or service. The appellant should include with their redetermination request any.
Po Box 7861 Madison Wi 53707 Fill Online, Printable, Fillable, Blank

Transferring your appeal rights to your provider or supplier so they can file an appeal if medicare decides not to pay for an item or service. There are 2 ways that a party can request.
Medicare 99204 Reimbursement 2024 Myrle Ortensia

Please complete each field on the form to ensure accurate processing. If you received a medicare redetermination notice (mrn) on this claim do not use this form to. Transferring your appeal rights to your provider.
Redetermination/Reopening Form Tutorial JF Part B Noridian
Medicare part b je redetermination form please submit one claim per redetermination request form. Do not complete this form for the following situations: The appellant should include with their redetermination request any and all documentation.
Fillable Online Request for redetermination of a Part B claim for

You may also submit additional evidence at a later time, but all evidence must be received prior to the issuance of the redetermination. Please complete each field on the form to ensure accurate processing. Medicare.
Fillable Online Medicare Part B JE Redetermination Form Fax Email Print

There are 2 ways that a party can request a redetermination: Please attach the evidence to this form or attach a statement explaining what you intend to submit and when you intend to submit it..
Medicare part b redetermination form Fill out & sign online DocHub

Please complete each field on the form to ensure accurate processing. Please attach the evidence to this form or attach a statement explaining what you intend to submit and when you intend to submit it..
Medicare redetermination fillable form pdf Fillable forms, Medicare, Form

Get forms to appeal a medicare coverage or payment decision. There are 2 ways that a party can request a redetermination: An * denotes a required field. Medicare part b redetermination and clerical error reopening.
If you received a medicare redetermination notice (mrn) on this claim do not use this form to. You may also submit additional evidence at a later time, but all evidence must be received prior to the issuance of the redetermination. Get forms to appeal a medicare coverage or payment decision. Medicare part b je redetermination form please submit one claim per redetermination request form. If you received a medicare redetermination notice (mrn) on this claim do not use this form to request further appeal.
Please attach the evidence to this form or attach a statement explaining what you intend to submit and when you intend to submit it. If you received a medicare redetermination notice (mrn) on this claim do not use this form to. You may also submit additional evidence at a later time, but all evidence must be received prior to the issuance of the redetermination. Please attach the evidence to this form or attach a statement explaining what you intend to submit and when you intend to submit it.
The Appellant Should Include With Their Redetermination Request Any And All Documentation That Supports Their Argument Against The Previous Decision.
Medicare part b je redetermination form please submit one claim per redetermination request form. Please attach the evidence to this form or attach a statement explaining what you intend to submit and when you intend to submit it. If you received a medicare redetermination notice (mrn) on this claim do not use this form to request further appeal. If you received a medicare redetermination notice (mrn) on this claim do not use this form to.
Please Complete Each Field On The Form To Ensure Accurate Processing.
There are 2 ways that a party can request a redetermination: Please attach the evidence to this form or attach a statement explaining what you intend to submit and when you intend to submit it. Get forms to appeal a medicare coverage or payment decision. Do not complete this form for the following situations:
You May Also Submit Additional Evidence At A Later Time, But All Evidence Must Be Received Prior To The Issuance Of The Redetermination.
An * denotes a required field. You may also submit additional evidence at a later time, but all evidence must be received prior to the issuance of the redetermination. Medicare part b redetermination and clerical error reopening request form. Transferring your appeal rights to your provider or supplier so they can file an appeal if medicare decides not to pay for an item or service.
Please Complete And Mail This Form With All Pertinent Documentation (Medical Records, Certificate Of Medical Necessity, Operative Notes, Advance Beneficiary Notice Of Noncoverage, Etc.).
Medicare redetermination request form department of health and human services centers for medicare & medicaid services 1.
There are 2 ways that a party can request a redetermination: If you received a medicare redetermination notice (mrn) on this claim do not use this form to. An * denotes a required field. Medicare redetermination request form department of health and human services centers for medicare & medicaid services 1. Medicare part b je redetermination form please submit one claim per redetermination request form.