
Medi Cal Choice Form Online
Medi Cal Choice Form Online - For a list of translated mced forms by language, please click on the following link: California department of health care services • health care. You will also learn what you must. Easily fill out pdf blank, edit, and sign them. See the provider directory for doctor/clinic codes. Applications are available in english and other languages. You are an immediate family.
You were a previous kaiser permanente member in the last 12 months; Save or instantly send your ready documents. See the provider directory for doctor/clinic codes. For food, cash aid, and health coverage.
Solicitud para el programa de pago de primas de seguro de saluddepartment of health care services For a list of translated mced forms by language, please click on the following link: California department of health care. Send your completed and signed application to the address. You were a kaiser permanente member in the last 12 months; You may be eligible to enroll in kaiser permanente if you meet one of these requirements:
Medi cal renewal form Fill out & sign online DocHub

See the provider directory for doctor/clinic codes. You will also learn what you must. Save or instantly send your ready documents. You may be eligible to enroll in kaiser permanente if you meet one of.
Medical Choice Form ≡ Fill Out Printable PDF Forms Online

Solicitud para el programa de pago de primas de seguro de saluddepartment of health care services You were a kaiser permanente member in the last 12 months; Use this form to join or change health.
Fillable Online MediCal Choice Form for Los Angeles County Fax Email
You may qualify to join kaiser permanente health plan if you meet one of these requirements: For food, cash aid, and health coverage. You are an immediate family. Even if you’ve been denied recently, you.
FREE 9+ Sample Medical Choice Forms in PDF MS Word

For food, cash aid, and health coverage. California department of health care services • health care. Send your completed and signed application to the address. California department of health care. Fill in the ovals to.
MediCal小冊子 『My MediCal Choice For Healthy Care』大解説 ドクターの選択とフォームの記入

Benefits will not change for voluntary beneficiaries who remain in. You were a kaiser permanente member in the last 12 months; California department of health care services, p.o. California department of health care. Solicitud para.
Medi Cal Renewal Form 2023 Printable Forms Free Online

Benefits will not change for voluntary beneficiaries who remain in. Easily fill out pdf blank, edit, and sign them. You will also learn what you must. Choose a plan and a plan partner from the.
Medi Cal Choice Form Doctor Clinic Code

Even if you’ve been denied recently, you may be eligible now. You are an immediate family. Save or instantly send your ready documents. You were a kaiser permanente member in the last 12 months; Applications.
california choice forms

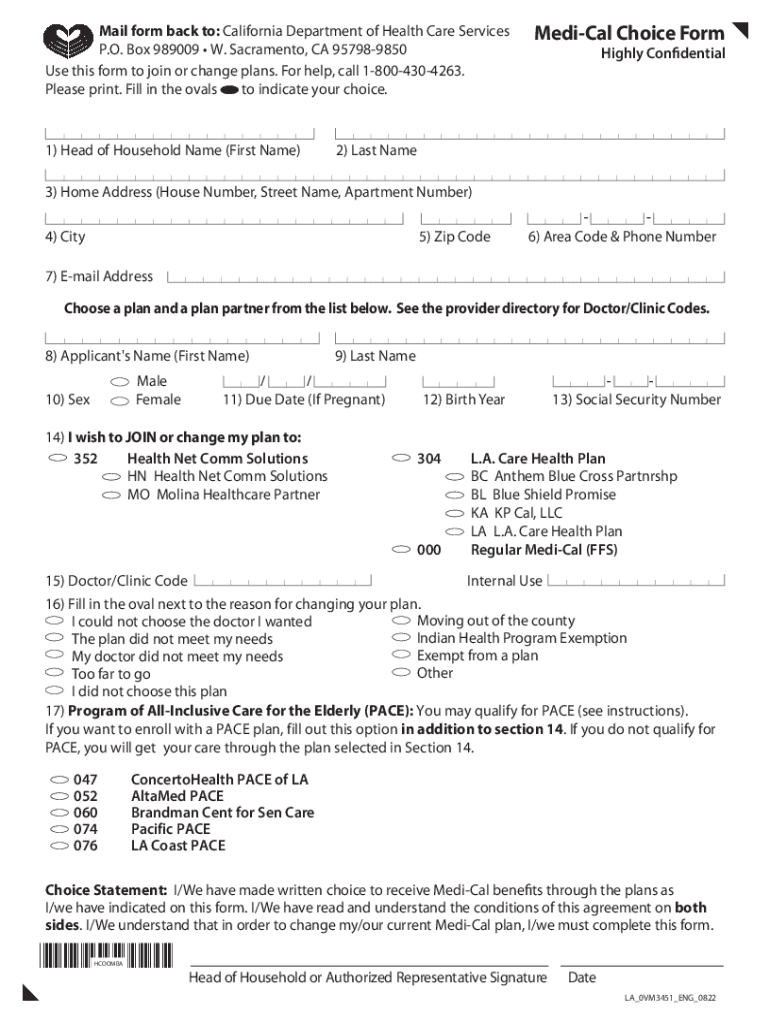
Use this form to join or change health plans. You will also learn what you must. California department of health care services • health care. California department of health care. For food, cash aid, and.
Benefits will not change for voluntary beneficiaries who remain in. You may qualify to join kaiser permanente health plan if you meet one of these requirements: You were a previous kaiser permanente member in the last 12 months; Fill in the ovals to indicate your choice. California department of health care services, p.o.
Use this form to join or change health plans. Choose a plan and a plan partner from the list below. You were a previous kaiser permanente member in the last 12 months; Send your completed and signed application to the address.
Easily Fill Out Pdf Blank, Edit, And Sign Them.
Solicitud para el programa de pago de primas de seguro de saluddepartment of health care services You are an immediate family. California department of health care services, p.o. Send your completed and signed application to the address.
Applications Are Available In English And Other Languages.
See the provider directory for doctor/clinic codes. California department of health care. Benefits will not change for voluntary beneficiaries who remain in. You will also learn what you must.
For A List Of Translated Mced Forms By Language, Please Click On The Following Link:
You may qualify to join kaiser permanente health plan if you meet one of these requirements: You were a previous kaiser permanente member in the last 12 months; Even if you’ve been denied recently, you may be eligible now. Save or instantly send your ready documents.
California Department Of Health Care Services • Health Care.
You may be eligible to enroll in kaiser permanente if you meet one of these requirements: Fill in the ovals to indicate your choice. Choose a plan and a plan partner from the list below. For food, cash aid, and health coverage.
You are an immediate family. Applications are available in english and other languages. California department of health care. Easily fill out pdf blank, edit, and sign them. Use this form to join or change health plans.